Autonomic Dysreflexia

What is Autonomic Dysreflexia?
Autonomic Dysreflexia (AD), sometimes referred to as Autonomic Hyperreflexia, is a potentially life-threatening medical condition that many people with spinal cord injury (SCI) experience when there is a pain or discomfort below their level of injury, even if the pain or discomfort cannot be felt.
Am I at risk for AD?
- People with injury levels at or above T6 are at risk for AD.
- Read Understanding Spinal Cord Injury Part 1 to learn about levels of injury at msktc.org/sites/default/files/lib/docs/Factsheets/SCI_Understand_Spin_Crd_Inj_Prt1.pdf.
- People with injury levels below T6 may also be at risk for AD in some rare situations.
Why do people with SCI get AD?
AD happens because there is a change in the body’s autonomic reflexes after injury.
Autonomic Reflexes before SCI
The autonomic nervous system controls body functions like blood pressure, heart rate, body temperature, sweating, digestion, sexual function, and dilation of your eyes’ pupils through signals sent back and forth from the brain and body through the spinal cord nerves. These functions are largely automatic or involuntary, meaning they are controlled without you thinking about it.
There are two main systems within the autonomic nervous system.
- Sympathetic nervous system – this is the body’s involuntary “fight or flight” response to prepare the body for action when there is some type of stress or threat. Pupils are dilated; the heart rate increases; the heart pumps with more force; and blood vessels get narrower causing blood pressure to rise.
- Parasympathetic nervous system – this is the “rest and digest” response. It causes digestion to improve, the heart to pump more slowly and with less force, and blood vessels get wider causing blood pressure to lower.
The body’s first reaction to pain or discomfort is to go into the sympathetic, “fight or flight” mode. However, the brain usually reacts quickly and sends a parasympathetic, “rest and digest” response to counteract the sympathetic response. This normally creates the balance needed to prevent the body from overreacting to any pain or discomfort and staying in that “fight or flight” mode.
Autonomic Reflexes after SCI
Your body’s first reaction to pain or discomfort below your injury level is still to go into the sympathetic, “fight or flight” mode. Your brain then tries to send the parasympathetic, "rest and digest" response to counteract the sympathetic response, but your SCI blocks the signals from reaching the spinal cord below your injury level. The "rest and digest" response only reaches those areas above your injury level, and this allows the “fight or flight” mode to continue out of control below your injury level.
Why is AD life-threatening?
AD is life-threatening because blood pressure can rise to dangerous levels when your body stays in that “fight or flight” mode.
Blood Pressure before SCI
The heart pumps blood to all parts of the body via blood vessels called arteries. Blood pressure is the force of the blood as it pushes against the walls of the arteries.
Blood pressure is always given as two numbers.
- Systolic (top number) is the pressure in the arteries when the heart squeezes to pump blood.
- Diastolic (bottom number) is the pressure in the arteries when the heart relaxes.
Most people have a normal baseline blood pressure of about 120mmHg/80mmHg. Blood pressure changes depending on what a person is doing. For example, blood pressure can be higher during exercise or when a person is in pain. Blood pressure can be lower during rest or sleep. The brain monitors these changes and uses the autonomic nervous system to keep blood pressure in balance.
Blood Pressure after SCI
Blood vessels around the bowels, which represent a large portion of the circulatory system that influences overall blood pressure, are controlled by nerve signals below T6. This is why people with injuries at T6 or above have difficulty keeping blood pressure in proper balance.
- Baseline blood pressure may be lower for some people with SCI, somewhere around the 90−110mmHg/50−60mmHg range.
- AD occurs when a pain or discomfort somewhere below the T6 level of injury causes your systolic blood pressure to rise 20mm to 40mm higher than your normal baseline or your diastolic blood pressure to rise 15mm to 20mm higher than your normal baseline.
- Your blood pressure will continue to be high until the cause of the pain or discomfort is resolved. If not, the rise in blood pressure can lead to uncontrolled high blood pressure emergencies (hypertensive emergencies).
- Hemorrhagic stroke (a rupture or leak in a blood vessel in the brain)
- Organ damage (heart attack, heart failure, kidney failure)
- Seizures (changes in the brain’s electrical activity)
- Death
What can trigger AD?
AD can be triggered by anything that might normally cause pain or discomfort below your level of injury even if you cannot feel the pain. Here are the most common areas of concern.
- Bladder (#1 cause of AD) – the bladder is full and needs to be emptied. People who use indwelling (Foley) catheters, condom catheters (sometimes referred to as sheaths) or suprapubic catheter usually have a kink/blockage of urine flow causing the AD.
- Bowel – constipation, flatus (gas), bowel needs emptying, or hemorrhoids are inflamed.
- Skin – there is a pressure ulcer, pinched skin, cut, ingrown toenail, something too hot or cold touching the skin, or another problem.
- Broken bone
- Sexual activity
- Menstruation (women)
What are the symptoms of AD and how do I know if I am having it?
The symptoms of AD are caused by the rising blood pressure. Symptoms vary from person to person, and there are some reports of no symptoms but high blood pressure during urination, bowel programs, bladder studies (urodynamics), and sperm retrieval. However, people usually experience one or more symptoms that are fairly easy to recognize.
- Pounding headache
- Sweating above the level of injury
- Slow pulse (although rare, a fast pulse can occur)
- Goose bumps
- Skin redness or flushing
- Nasal congestion
- Chills without fever
- Blurred vision
- Restlessness
- Cold and clammy skin below the level of injury
What do I do if I have AD?
Most people with a T6 level of injury or above experience AD after injury. They also learn to recognize symptoms and know it is important to quickly act to find the source of the problem and fix it. Here is a checklist you can follow to resolve AD whenever you are experiencing it. Get help from a caregiver if needed.
- Check your blood pressure. Everyone at risk for AD needs to have a home blood pressure monitor and know how to use it.
- Check your blood pressure about every five minutes while you try to find the cause of the AD episode.
- If your systolic blood pressure is greater than 150 mmHg, then consider using some medication to lower it. Nitropaste applied to the skin above the level of injury is most commonly recommended. Wipe off the nitropaste once blood pressure is stable. Caregivers should wear gloves when applying the medication.
- Find the cause of AD and fix the problem if you can.
- Sit upright.
- Loosen any tight clothing or anything else that might be tight fitting.
- Check to see if bladder is too full.
- Is your catheter tube kinked or a condom catheter on too tight?
- Does your bladder need emptying?
- Check to see if your bowel is full.
- If you have lidocaine gel, you can use it to numb the anal area before you check your bowel. This can help prevent causing more discomfort as you are checking.
- Check skin for a pressure sore, inflamed hemorrhoids, cuts, burns, ingrown toenails, or any other skin irritation.
- Check for broken bones.
- If you are unable to identify the cause of AD and/or control your blood pressure with the medications that you have, then you will need to seek medical attention. Call 911.
- Clip the card (at the end of the factsheet) to carry with you. Give it to medical professionals to assist them in treating AD.
Is there treatment for AD?
It is important to know what your baseline blood pressure usually is because it will help you know when you have AD and need to take action. AD will resolve if you follow the steps above to find the source of the problem and fix it. However, AD can occur without any obvious or easily treated cause and you may need to be hospitalized to manage your blood pressure while doctors search for the cause of the AD. Once you have identified the cause of an AD episode, you might need to make some changes in the way you do things to prevent future episodes.
Can I prevent AD?
Good ongoing personal care is the best way to prevent AD.
- Maintain a consistent bladder program and take necessary steps to prevent infections.
- Maintain a consistent bowel program.
- Check your skin daily for pressure ulcers, and do regular pressure reliefs (also called weight shifting, pressure redistribution and pressure reduction) to prevent pressure ulcers.
- Avoid other skin injuries such as cuts, bruises and sunburn.
- Make sure you wear loose clothing and avoid clothes and shoes that are too tight.
- Use good techniques and well-functioning equipment to minimize the risk of falls and injuries.
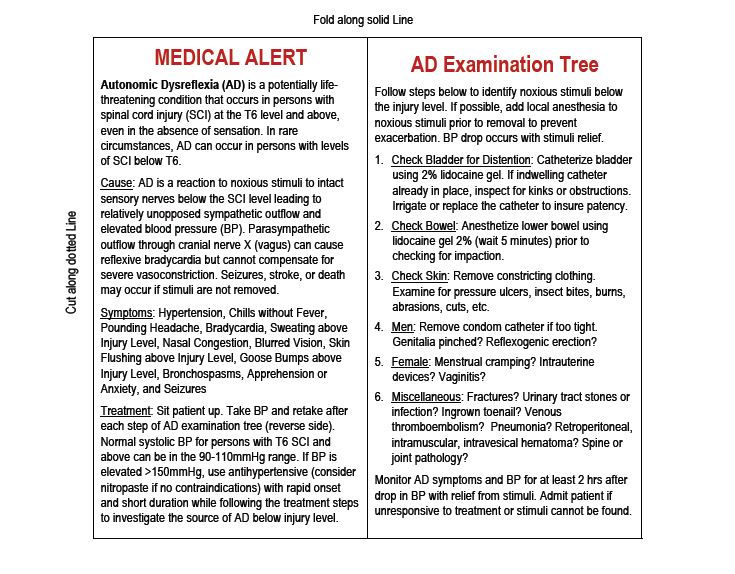
Keep this wallet card with you at all times. Give it to medical professionals to assist them in treating AD.
Authorship
Autonomic Dysreflexia was developed by Anthony Chiodo, M.D., Deborah A. Crane, M.D., Maria R. Reyes M.D., Shawn Song, M.D. and Phil Klebine, M.A., in collaboration with the SCI Model Systems Knowledge Translation Center.
Disclaimer: This information is not meant to replace the advice of a medical professional. You should consult your health care provider regarding specific medical concerns or treatment. The contents of this fact sheet were developed under a grant from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR grant 90DP0012-01-00). NIDILRR is a Center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this fact sheet do not necessarily represent the policy of NIDILRR, ACL, HHS, and you should not assume endorsement by the Federal Government.
Copyright © 2016 Model Systems Knowledge Translation Center (MSKTC). May be reproduced and distributed freely with appropriate attribution. Prior permission must be obtained for inclusion in fee-based materials.